Back in September 2025, US President Donald Trump and Health and Human Services Secretary Robert F. Kennedy, Jr. held a White House briefing linking Tylenol (acetaminophen, or paracetamol to Europeans) use in pregnancy to autism. A new study in The Lancet looks at what happened to acetaminophen prescriptions during emergency room encounters for pregnant females aged 15–44. They used data from a large database covering over 1,633 hospitals and 37,000 clinics.
Here is panel A from the figure in the study, with the vertical dashed line marking the date of the White House briefing (September 22, 2025) and the other dashed lined showing the expected prescribing rates (compared to the observed ones).
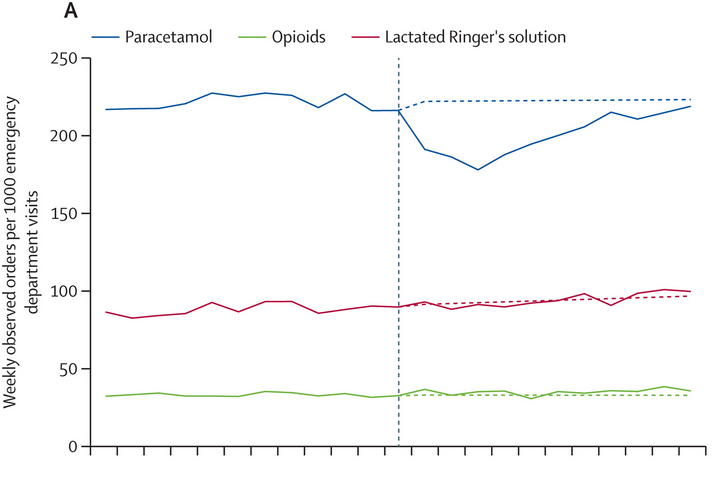
Following the briefing, acetaminophen prescriptions fell sharply:
During the initial study period, a 16% decrease (0·84 [0·81–0·86]) was measured, with a maximal change (20%) during the third week.
There is good reason to believe this sharp change is causal, as there was no contemporaneous change in acetaminophen prescriptions among non-pregnant females in the same age range, nor in the prescribing rates of the two comparator drugs:
There was no statistically significant change in emergency department paracetamol use among non-pregnant female emergency department patients aged 15–44 years, nor among the comparators, regardless of pregnancy status.
What you don’t see in the headlines of the stories reporting on this study is the fact that acetaminophen prescriptions recovered to close the expected level by the end of the study period (December 7). The authors have this to say about this observation:
Explanations for the waning change in paracetamol use in emergency departments include fading salience of the press conference […] and messaging from trusted organisations refuting claims made at the briefing. Paracetamol use also generally rises in late November due to the onset of cold and influenza season, and our model did not account for seasonality.
Annoyingly, this study tells us less than we hoped for, because they did not account for seasonality in acetaminophen prescribing to calculate the expected values in the post-briefing period, so we don’t know how much to attribute the recovery in prescribing to flu season versus the waning effect of the briefing (or something else). I’m not sure why they didn’t try to model seasonality. True, it’s not as simple as just looking at the previous year’s seasonality, since the timing and intensity of flu season varies. But I’m sure they have multiple years of data available to give us some idea of the connection between the onset of flu season and acetaminophen prescribing in the ED. Maybe this would have taken their study beyond where they wanted to go, but it does leave us with a frustratingly incomplete picture of this unusual health intervention.